Background
Corrected transposition of the great arteries (TGA) is a rare condition often associated with other heterogeneous cardiac anomalies. [1] It has been estimated to account for 0.5-1.4% of clinically apparent congenital heart disease cases. [2, 3] Of this group, probably fewer than 1% of individuals have no associated abnormalities. [4] In corrected transposition of the great arteries, the left atrium is connected to a right ventricle, from which an aorta arises. Hence, two discordant connections occur in sequence. Congenitally corrected TGA can be diagnosed prenatally, and many patients require early surgical treatment. [1]
In 1875, Von Rokitansky first described this condition in two cases. In 1919, Weinberger first reported that it is fairly frequently associated with dextrocardia. [5]
Relevant Anatomy
Knowing the position of the atrioventricular (AV) node in this defect is extremely important if injury to it during surgery is to be avoided. Because of the L-looping of the ventricles in this condition, the usual posterior position of the AV node is prevented from reaching the interventricular septum because of the malalignment of the atrial and inlet ventricular septa. An anterior node is present, either alone or in addition to the posterior node, and it is located in the floor of the right atrial wall immediately anterolateral to the interatrial septum. This gives rise to an AV bundle that penetrates the fibrous annulus to make contact with the ventricular myocardium. It then passes anterior to the pulmonic annulus along the morphologic left ventricular side of the septum and subsequently courses anterior and superior to a perimembranous outlet ventricular septal defect (VSD). [6, 7]
This anterior position of the AV node is more commonly reported in situs solitus. In situs inversus, a posteriorly positioned AV node has been described. [8] However, other authors stress that either position of the AV node is possible with any situs. [9]
The coronary arteries arise from the aortic valve sinuses adjacent to each ventricle. The morphologic left coronary artery arises from the right-sided posterior sinus, and the morphologic right coronary artery arises from the left-sided posterior sinus. The most common coronary artery abnormality is a single coronary artery that arises from the right-sided posterior sinus. [10]
Problem
The presence of ventricular inversion (ie, atrioventricular discordance) with ventriculoarterial discordance has been called corrected transposition or physiologically corrected transposition because these two anomalies in sequence ensure that blood flow continues in its usual physiologic pathway. However, because this condition is usually associated with other abnormalities, many have commented that it should not be called corrected. [11, 12]
The four chambers of the heart have distinct features that identify them regardless of their actual spatial location or connection. Therefore, even if a ventricle is present on the left side, it can be identified as a morphologic right ventricle. The right ventricle is identified by the presence of a muscle tissue that traverses it horizontally near the apex (ie, moderator band) and by the tricuspid valve, which is situated more apically than the mitral valve at its attachment to the crux of the heart. Also, the tricuspid valve has multiple papillary muscle attachments to the septum (unlike the mitral valve, which has none) and is separated from the pulmonary valve by the muscular band of tissue called the crista supraventricularis or conus. The broad triangular shape of the right atrial appendage assists identification of the right atrium because it is different from the narrow, fingerlike left atrial appendage.
In the nomenclature advocated by Van Praagh in 1989, this form of transposition has been designated S,L,L. [13] The S stands for atrial situs solitus, indicating that the morphologic right atrium lies to the right of the morphologic left atrium. The first L is for an L-looped right ventricle or a right ventricle with a left-hand pattern of internal organization. During the process of development in a normal heart, the right ventricle comes to lie on the right side so it undergoes a dextro-loop (ie, d-loop). A d-loop ventricle is one in which the internal pattern of the right ventricle conforms to a right-hand pattern, in which an extended thumb indicates the attachment to the tricuspid valve and in which the fingers indicate the right ventricular outflow tract when the palm is placed on the septal surface. The second L stands for the position of the aortic valve, which is anterior and to the left of the pulmonic valve.
In the normal heart, the aorta is posterior and to the right. In the presence of situs inversus, the nomenclature for corrected transposition is I,D,D. In a detailed study on the pathologic anatomy in 34 specimens with corrected transposition and two ventricles, Van Praagh et al found that the segmental classification was S,L,L in 94%, I,D,D in 3%, and S,L,D in 3%. [14]
Pathophysiology
Pathophysiology is determined by the presence and type of associated lesions. When no other defects are present, the path of the blood flow is physiologic; blood from the left atrium enters the right ventricle and is then directed into the aorta, and, on the right side, the deoxygenated blood from the vena cava enters the left ventricle. Because of the ventriculoarterial discordance, the deoxygenated blood is then directed into the pulmonary artery. Thus, the oxygen saturations in the heart chambers and in the great arteries are normal.
The most common anatomic associations include the presence of a ventricular septal defect (VSD), which may be observed in almost 80% of cases and the presence of pulmonary stenosis, which has been reported in approximately 50% of cases. [4, 15] The presence of a VSD causes a systemic-to-pulmonary shunt; however, this is usually balanced because of the protective effect of coexisting pulmonic stenosis.
Tricuspid valve anomalies, including dysplasia, straddling, or Ebstein-like malformation (with or without regurgitation) are also quite common and are reported in 14-56% of patients. [15, 16] Tricuspid regurgitation in this setting of a systemic ventricle, which is the morphologic right ventricle, is much more ominous than it would be in an otherwise normal heart. Coarctation and interrupted aortic arch have also been frequently reported, but subvalvar and valvar aortic stenosis are quite uncommon. [12, 15] Conduction abnormalities also are common. The reported incidence of complete atrioventricular (AV) block has ranged from 12-33%. [17, 18] Spontaneous progression of AV block has been reported to occur at a rate of 2% per year. [17, 19] Additional rhythm problems include Wolff-Parkinson-White syndrome, supraventricular tachycardia, atrial flutter, and atrial fibrillation. [2, 16, 18]
Etiology
As with almost all forms of congenital heart disease, the causes are thought to be multifactorial. Most of the clinical and surgical retrospective studies have reported a male predominance in corrected transposition. [15, 16] One study suggested an autosomal recessive mechanism of transmission may be present in some families. [20] Interestingly, they found that transposition of the great arteries was the most common recurrent defect in families with congenitally corrected transposition, suggesting a pathogenetic link between these two entities.
Presentation
Patients with isolated corrected transposition of the great arteries may present in adulthood because of abnormal radiography or ECG findings and may have no symptoms, at least for the first 3 or 4 decades of life. See the image below.
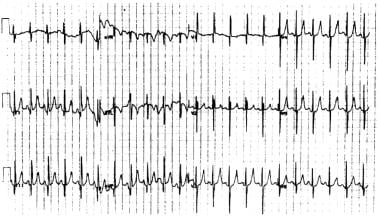 Surgical Approach to Corrected Transposition of the Great Arteries. A 12-lead electrocardiogram demonstrates the characteristic features of corrected transposition Q waves in III, in aVF, and in the right precordial leads.
Surgical Approach to Corrected Transposition of the Great Arteries. A 12-lead electrocardiogram demonstrates the characteristic features of corrected transposition Q waves in III, in aVF, and in the right precordial leads.
In a study of 18 patients, Presbitero et al found that rhythm disturbances and tricuspid regurgitation were present more frequently after the third decade of life. [21] They found that this and impaired right ventricular function developed in 66% of patients older than 50 years, causing congestive cardiac failure.
A multi-institutional study confirmed that congestive cardiac failure is common in patients with or without associated cardiac defects. [22] By age 45 years, 67% of patients with associated anomalies and 25% of patients without associated anomalies were in congestive cardiac failure.
Another large study by Rutledge et al confirmed that survival rates are reduced in these patients. [23] They found poor right ventricular function and complete AV canal as risk factors for mortality. Risk factors for progressive right ventricular dysfunction included conventional biventricular repair, complete AV block, and severe tricuspid regurgitation.
Most patients who have associated anomalies present in infancy with a murmur or heart failure. Patients with bradycardia secondary to complete AV block can present at any age. Unless these patients have pulmonary atresia or severe pulmonic stenosis, cyanosis is not present. An important physical finding is the presence of a loud single second heart sound along the upper left sternal border.
Indications
For the rare patients who have corrected transposition and no other associated abnormalities, no treatment may be required because their life expectancy has been reported to be near normal. [24, 25] Presently, the treatment of patients with associated anomalies is predicated on the presence of symptoms (eg, heart failure) caused by a moderate ventricular septal defect (VSD) or on significant objective deterioration, if present, such as progressive right ventricular dilatation, severe tricuspid regurgitation, or complete heart block with a slow escape rate. [26]
The surgical management of even the simple associated defects, such as a VSD or pulmonic stenosis, has been reported to be associated with much higher morbidity and mortality rates in these patients than would occur in a patient with an otherwise normal heart. Furthermore, these procedures may not result in a functional improvement. Also, technically, the approach to address the VSD or the pulmonic stenosis is difficult, and the risk of surgically induced complete heart block is quite high. [26]
Contraindications
Patients with corrected transposition and no other associated abnormalities may not require treatment because their life expectancy has been reported to be near normal. [24, 25] However, no clear consensus has been reached regarding this group of patients at this time. At the other end of the spectrum, a double-switch procedure, as described below, would be contraindicated in patients with severe hypoplasia of either ventricle. These patients should be considered for a Fontan-type repair.
-
Surgical Approach to Corrected Transposition of the Great Arteries. A 12-lead electrocardiogram demonstrates the characteristic features of corrected transposition Q waves in III, in aVF, and in the right precordial leads.
-
Surgical Approach to Corrected Transposition of the Great Arteries. An anteroposterior chest radiograph reveals the straightened left heart border formed by the aorta, which is more leftward and anterior than usual.
-
Surgical Approach to Corrected Transposition of the Great Arteries. A transthoracic echocardiogram in the apical four-chamber view illustrates the moderator band in the left-sided ventricle and the apically displaced left atrioventricular valve, suggesting that it is the morphologic right ventricle.
-
Surgical Approach to Corrected Transposition of the Great Arteries. A transthoracic echocardiogram in the parasternal short axis view demonstrates the anterior and leftward aorta. The left coronary artery can be observed at the 10-o'clock position.





